HOW NOT TO DIE
- Jun 1
- 54 min read
Updated: Jun 16
I’m declaring 2026 the year of the moral panic. We’re really going all-in, here. Aren’t we? To me, the following is quickly becoming Canada’s Epstein files: replete with the wildest allegations accompanied by a shocking paucity of evidence and a growing international furor all due to reporters, journalists, and editors showing no willingness to ask the most obvious questions or offer readily available data while, of course, delivering outlandish headlines.
— Now, what follows is 13,700 words covering all manner of cases and themes relating to death, dying, euthanasia, and suicide, with a focus on Canada's MAiD program. If you don’t want to read about that then here is a good place to turn away. As evidenced in this essay, if you or someone you know is struggling with mental health issues or thinking about harming yourself there really are folks all over with backgrounds, expertise, and resources or every sort who want to help.
TL;DR
The quality of the conversation around dying and medically assisted dying is atrocious.
Except for a few radicals, almost everyone is for medically assisted dying: as long as it uses their preferred euphemisms, is administered by their people, and avoids circumstances they're personally uncomfortable with.
Those most vocal in their opposition to Canada's MAiD don't offer great arguments and avoid obvious comparisons. They also love providing unverifiable instances and non-existent hypotheticals and like to misrepresent or straight-up lie about MAiD and the people who've sought it out.
No, Canada does not resemble Nazi Germany but does, kind of, operate its assisted dying program a little bit like present-day Belgium and Netherlands (if you squint your eyes and tilt your head sideways.)
MAiD does not look like a get-rich-quick scheme for Canadian doctors.
The suicide rate in Canada is lower than at any time in generations while organ donation is middling; the rate of MAiD deaths is not crazy and organ donation by MAiD recipients is moderate, making up only a small percentage of overall donations.
Canada's medical system, like its MAiD program, has plenty of room for improvement but is not terrible and aligns with peer nations on most fronts (unlike the US).
Since when did Americans and Brits care so much about Canadian policy or social issues? Why is all this furious reporting and podcasting (that must have taken weeks or months to organize, conduct, edit, and publish) all arriving around the same time?
Why not upgrade the conversation and talk about real stuff and what's actually happening?
CHAPTER I - OFFERED?
A SERIOUS ALLEGATION
The Western Journal and others “reported” [sic] on April 6th, 2026, “Woman with Back Pain Horrified at ER Visit, Says Doctor's 'Very First Words' Offered Her Euthanasia.” I hope we all agree that’s a shocking allegation. The trouble is that it doesn’t look to me like this happened. Why? Many reasons. To start, this 84-year-old, Miriam Lancaster, had not filed a complaint or even taken her allegation to the press (regarding an event she says transpired a whole year prior) but, instead, religiously-inspired papers plucked the story off a post from this woman’s Facebook page. When she did officially come out with the story she published it in the press, again, rather than spelling out her situation, naming people, and submitting a formal complaint.

The backstory we’re given is that Lancaster was getting out of bed one morning, put her foot on the floor and had such excruciating and unusual pain that she cried out. It is unclear to whom she called. What we do know is that paramedics showed up and she was whisked off to emergency. Her daughter tells these non-adversarial reporters that “we just wanted pain relief. And we wanted to know what had happened. It was difficult to identify where the pain had come from.” And we know that after some tests doctors found the source of the pain was a fractured sacrum — which is typically treated with bed rest. Lancaster also reports that while she healed in hospital (for how long we do not know but 3-6 weeks is common) she received excellent care. So she took up the time of emergency responders, the crew at a busy urban ER, and a bed in an overwhelmed hospital when what she, a frail senior with serious osteoporosis who has outlived median life expectancy, needed was extra strength Tylenol, maple walnut ice cream, and some Netflix.
Neither Ms Lancaster nor her daughter or any family members (nor her family doctor or lawyer, spiritual advisor or church community, friends or neighbours, or anyone else) made a formal complaint of any kind against any individual or organization at the time of the incident or in the year since. That would seem like the minimum you would do, wouldn’t it? After all, together the woman and the press are, in effect, claiming and acting as if Lancaster narrowly escaped a murder attempt. That's how they're framing this. And yet, no one even did so little as identify any person involved or even leave any potentially identifying hints in all of this reporting, either; thus, no one could check any details or hear any another side of this story, and enough time elapsed that any recollection was unlikely and probably poor at best.
Myself and everyone else, surely, are desperate to know which healthcare professional it was who was behaving so atrociously. And, given the seriousness of what's being alleged, why would the the victim get to preserve the perpetrator’s anonymity. Right? No one is claiming a discussion or end-of-life arose after 12 weeks in hospital, an endless battery of useless tests and ineffective treatments, and morphine failing to dull this woman’s unbearable pain. The allegation is that someone in the ER was positively eager for her to die the moment they saw Lancaster arrived in the ER. So, who is she protecting and why? Or is it more likely this whole thing is fiction?
Still, as a result of this weird selective silence and no journalistic probing of any sort, no real inquiry was able to happen. As you would expect, however, Vancouver Coastal Health did feel the need to respond to this allegation, however vague, and look into it. They publicly stated that they’re not aware of any such conversation between the victim and staff in the emergency department at Vancouver General Hospital. So, something isn’t right with this story and reporting on it without digging for further obvious and needed details seems to me like a clear dose of journalistic malpractice on top of the alleged medical malpractice.
AGAIN, AGAIN!
A month later, on May 4th, 2026 The Catholic Herald told us (based on “reports” from Eternal Word Television Network, Inc. Irondale, Alabama) that a Vancouver priest, Father Holland, was offered euthanasia while recovering in hospital. More than that, they insist the devout Catholic “was twice offered assisted death by hospital medical staff who knew he was a priest and opposed to euthanasia — a practice critics say is growing.”
In this and other reporting, Father Holland described his feeling about this, telling us “I think I was very shocked. It is such a sensitive subject … There are some things you just don’t talk about to some people.” We're also told the priest explained to hospital staff that he was fundamentally opposed to assisted suicide (self-administered) or voluntary euthanasia (clinician-administered) and also that the doctor responded by telling him “he just wanted to make sure that, if a terminal diagnosis came up or not … I knew of the different services I had access to.” The article explains how, a few weeks later, still in hospital, Father Holland was “offered” euthanasia a second time and that this time the topic came up with a nurse.
BUT DID THAT HAPPEN?
That’s a set of wild claims, or mostly twisted framing as I see it. The first thing worth noticing is that, though he is quoted several times, not once does the alleged victim report being “offered” assisted suicide. At the very minimum, we should read such a serious allegation coming direct from the mouth of the victim, even just one time. Shouldn’t we? Then, it’s not just that what I hope we all interpret as very serious allegations were made and spread far and wide (ones asserted by the article’s author but unstated by the alleged victim) but that those doing the reporting sought neither to identify anyone nor, seemingly, to get verification or any other version of events from multiple parties involved. If there is any validity to the assertions in the article (or even the man’s rather different stated allegations) you would think the victim would wish to stop this from happening to others. You might even think, as I do, as suggested in the previous case, that such threats to vulnerable people, really no different than threats toward children or hate motivated ones toward minorities, have no place in society and are sufficiently serious that making such an allegation, privately or so publicly as this, obviously precludes the victim’s desire to protect the perpetrator(s). I mean, if you go to the press telling them that a police officer, lifeguard, or nurse approached you and asked if you would like for them to kill you, I hope someone somewhere at some point thinks to ask for a name, badge number, or mere description and public voices and institutions seek a transparent investigation. Surely someone would wish to learn something about the incident. Surely!
But, as ever, no doctor or nurse is named and no complaint or call for an inquiry was made at any time by anyone to any relevant authority. And, critically, the simplest bit of all is absent. No one even sought details about the man’s stay or the totality of his health situation, either; that is, other than a picture of a rather frail looking elderly man, in glasses and all white hair (and with a bad bruise on his arm) in a gown and lying on a hospital bed. Though there’s no caption, we can safely assume the photo is of Father Holland. (Oh, and that picture is paired with a provocative stock image, of a similar looking man in a darkened hospital room, the foreground of which is a hand gloved in blue surgical latex holding an ominous looking needle.) Father Holland and friends want us to imagine creepy doctors (probably crowned in devil’s horns) slithering around the halls of all our hospitals with needles filled with death and trying to trick people, Catholics especially, into signing away their souls and accepting Satanic injections. And they offer up a picture of their loony fiction for added realism.

If real reporting was to take place (and this wasn’t an obvious piece of propaganda) the patient may have been asked any number of questions about their experience or conduct in hospital or that of the staff. They may have been asked about some context at all. Given that seniors who’ve had hip surgery or full hip replacement are typically out of hospital in just a couple of days, it seems pertinent to enquire why this elderly man reports that he was still immobilized in bed in the offending hospital, overflowing with what we are told are perfidious practitioners, after many weeks. How long was he there? Three weeks? Nine? 32? Seems like he was far more frail and in a worse way than 99% of people with the condition he was being treated for. Regardless, Father Holland offers us nothing. The article just says that after the topic of MAiD was brought up the first time, presumably not prior to surgery, “a few weeks later” the topic came up again. It could be relevant to the story to learn whether the patient was relentlessly complaining that they were in excruciating pain and/or unable to walk, stand, sleep or eat, even after being dosed with increasingly serious analgesics. Did he come down with a secondary infection? Pneumonia or urinary tract infection, as is so common to stays in hospital? Does he have a frail heart, no kidneys, and a chronic blood condition? I can think of all kinds of questions I would ask to all kinds of people to help illuminate what precipitated what the patient tells us was an obviously unwanted conversation. None of that seems to have happened.
BASELESS BACK-UP
However, the article goes further. Father Lynn, friend of Father Holland and someone they describe as the ‘archdiocese’s pro-life chaplain’, offered to the Catholic press that this case “must surely be among the most appalling examples of Canada’s coercive and insensitive euthanasia regime.” And he tells us “It places the medical practitioner into the role of the devil, tempting a vulnerable person into mortal sin.” The author of the article then adds that all of this coercion and enthusiasm toward mortal sin is taking place “as Canada approaches 100,000 assisted dying deaths.”
Though this is a refrain you can find all over the place, they leave out that the MAiD option has been available for a decade and while knowing, of course, that there have been just 76,000 people in that time who happily took this option over the alternatives they were facing. Current numbers only show through 2024. Though we might wish to project 90,000 total deaths or 110,000 or more by the end of 2026, but that would only be a bad guess as annual numbers over the last decade have ranged from 1,000 to 16,500. They also offer their inflated figure knowing the vast majority of MAiD recipients are terminally ill seniors who are very likely in their last period of life, even if they were perfectly healthy, with a median cohort age close to the national median life expectancy. Father Holland, for instance, is 79 and life expectancy for males in Canada today is 80. If he were 104 he would, doubtless, still oppose MAiD and others would oppose him taking the option and even rile against the possibility. For added context (bold, I know), Holland was born in 1947 when life expectancy was just 64; so, safe to say he has experienced vastly more life than the majority of his predecessors and many of his peers as well (and both of my parents) and, as such, having a serious discussion about end-of-life with a medical professional outside his community and in a private, professional medical setting is not, as insisted, some wild, newsworthy event.
The intrepid reporter also neglects to mention that, as big as this number seems to them, there were many more folks seeking MAiD: who freely chose to back out after their application went through but before they received their meds; who died after applying but before approval or administration; or who were rejected for not meeting the necessary criteria. Knowing that, to me, this hardly looks like the mass murder regime it’s being painted as.
Without any comparisons offered for contrast or scale, the reader is also not reminded that in this same decade Canada saw a similar number of overdoses, just of opioids alone, and mostly of working-aged males in their prime. One of these situations, if you ask me, is a real social and moral crisis. They also fail to contrast their number with, for example, the fact that a whole decade of thankful and legal MAiD deaths is far fewer than a single year of cancer deaths, according to the Canadian Cancer Society, who tells us there are more than 240 cancer deaths per day or 87,000 per year in this country. So, though terminally ill cancer patients are the largest cohort of MAiD deaths, few people who are on their deathbed because of cancer take the MAiD option. Again, this doesn't look like we have a pre-mature or coerced death crisis on our hands.
Reporters and their MAiD antagonist friends also don’t want you to know or consider that 28,000 Canadians die annually from preventable healthcare-related errors and that this is “a leading cause of death in Canada”; or that, in addition to that, more than 10% of all hospital stays result in patients being gifted with infections, yielding over 220,000 cases and another 8,000 deaths each year. Right. So 36,000 people seeking health and life each year are killed by people intending to heal them. So that “help” looks like far more misery and mortality, and should be far more offensive, than any and all MAiD deaths. And if those details are absent then you wouldn’t expect reporters to remind people of the pandemic, either. They certainly don’t make space for a paragraph noticing that largely preventable, airborne infections decimated the same over-65 cohort who make up the bulk of willing MAiD recipients, killing over 58,000 in just four years — far too many of whom were gifted the virus by healthcare staff in care homes and hospitals or were entirely abandoned when their critical caregivers fell ill, leaving them in squalor and/or to die from dehydration, starvation, or injuries. (Just to drive this under-reported point home, more than five years later there has still been no national inquiry into the deaths of long-term care residents in Canada who accounted for ~80% of deaths during the first COVID wave, the worst performance among peer nations. Instead, we’re reporting on some people not being offered or receiving MAiD…)
Even if they framed all MAiD cases as egregious violations, which they mostly don’t, and aren’t just highlighting a few related instances they find questionable, the situation still looks nothing like it is presented as. At the least, I would imagine anti-MAiD activists would understate the total number of MAiD deaths to make the mistakes, terrible violations, or offending “offers” seem out of proportion and far beyond expectation and not, as they appear to me, far below normal and plausibly unavoidable cases of medical error. To me this is like being outraged at and endlessly reporting on a traffic accident, one in which no one was harmed all while framing that as evidence of the West's moral bankruptcy and resulting from a decline in religiosity. Why is that a terrible analogy and how does this case seem to you?
THE REAL DEAL
I think all this should make you wonder why, if they truly wished to save lives, these folks are wasting their time with their anti-MAiD activism and aren’t instead taking on surgical errors and complications, drug resistant infections and the overuse of antibiotics, hospital and care home air quality, and getting everyone who is unwell or treating the unwell in N95s… And perhaps that exposes the plot. These folks, our Catholic Fathers, aren’t concerned in the least with saving lives or reducing misery at all, are they? Their primary interest isn’t in the living of the Earth but with souls in the afterlife. As such, any amount of terrestrial suffering and death is tolerable and, in fact, seen as nothing at all in light of what they tell us is an eternal afterlife. And is there any doubt that this is how the anti-MAiD community justifies seeking to steal away people's hard-earned autonomy and eliminating their only ability to reduce their own suffering in a safe, supervised, and legal manner and with their loved ones present?
In all, as presented, this case reads to me like the devout Catholic was offended that anything related to this topic came up in his presence and very much less like, as it is being framed, as the man being “offered” death (which he never claims) nor even being tacitly encouraged to question, never mind abandon, any of his longstanding religious beliefs or otherworldly aims. As such, too, there appears to be exactly zero coercion here, either. And, as with the previous case, without any fingers actually being pointed or anyone with anything to lose coming forward on any side, it’s very hard for me to read this as anything but a religiously informed propaganda campaign from the mouths of the very people who tell us this is their business and who clearly have a whole spectrum of cosmic and earthly incentives to see MAiD restricted or shut down. (I keep offering this word propaganda here deliberately because the word originates with our Catholic friends, in the 17th century Congregatio de propaganda fide [Congregation for Propagating the Faith; aka Congregation for the Evangelization of Peoples, or the Dicastery for Evangelization], a Vatican department established by Pope Gregory XV to push Catholicism out to the world and manage global affairs with non-Catholics… And that’s exactly what all of this looks like to me.)
Aside from being absurd on its face, as far as I can tell, and though it is true that Health Canada documentation provides to those physicians and nurse practitioners involved in planning and consent for MAiD tells them they have a professional obligation to initiate a discussion about MAiD (not “offer” MAiD), Health Canada lacks the power to mandate any province or health authority adopt this guideline, of course; and, moreover, there’s no evidence I can find of any public agency or professional college in British Columbia, where Father Holland is, doing so.
And yet, as you would expect, a spokesperson for Vancouver Coastal Health had to respond to the media bluster and coming inquiries related to this case. They offered that their staff are “responsible for answering questions when patients bring up the topic of MAiD” and that those with the requisite knowledge, skills, and training are free to use their professional clinical judgement — in a relevant medical setting with people who could be eligible — and have a discussion. And we all know no professional, least of all someone in a hospital setting, is telling someone who came in for cataract or knee surgery that they are better off seeking medically assisted death. And if there was such an incident we all, MAiD proponents especially, want at minimum peoples’ names and a formal inquiry to follow, with serious life-altering repercussions for anyone engaged in what everyone considers serious malpractice. We might, then, ask why Catholic priests and other alleged victims, victims of those committing what we all consider professional malpractice and moral error, don’t want that? I have a guess.
THEN CAME A VIRAL HEADLINE
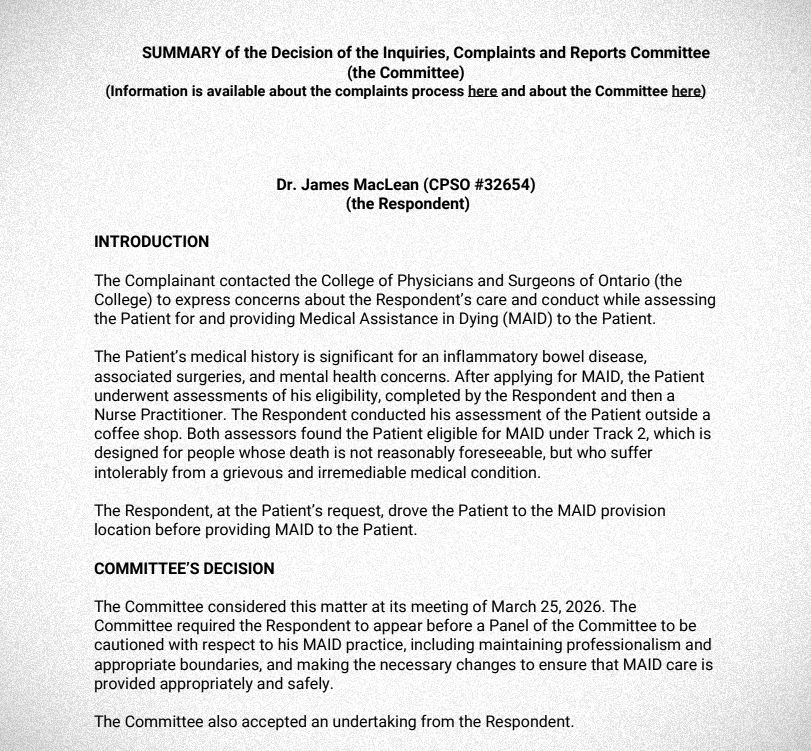
At the end of the month, on May 25th, 2026 we got an article from the National Post. The piece, titled “Ontario man dies of MAiD after being assessed outside Tim Hortons”, was picked up, reproduced, and shared seemingly everywhere. It went viral, really.

Like so many others, folks like Matt Walsh, the American conservative commentator, read the piece (presumably, though I wouldn’t bet on it) and reported to his millions of social media followers:
A doctor met a guy at a coffee shop, assessed him for MAiD, then drove him to the spot where he'd be put down. Horrors beyond comprehension happening just to our north. There's a much better moral argument for invading Canada and deposing its regime than invading or bombing any country 10 thousand miles away. Industrial scale eugenics and mass murder happening right next door.
Nice.
THE REALITY
Thomas Dillon (say his name) had a history of mental health issues, including persistent suicidal ideation and on-going problematic drug and alcohol use. He also had debilitating Crohn’s disease. Like almost anything, Crohn’s can be mild or severe and the worst symptoms can often be mitigated by surgery and/or daily medication — except when they can’t. Crohn's may cause severe chronic stomach pain accompanied with persistent diarrhea (a total nightmare) and may result in gut ulcers and fistulas. Common side effects include nutrient deficiency, chronic fatigue, kidney stones, sores and rashes, inflammation and more (total, total nightmare). For his bowel disease, Dillon underwent several associated surgeries, seemingly to insufficient benefit. And we’re told that because of his spectrum of illnesses he was unable to maintain a social network or personal relationships, he struggled to keep a job, and as a result was dependent on family for housing and financial support.
After applying for MAiD in 2023, this 45-year-old man waited seven months. Then in January of 2024 he underwent assessment for eligibility, completed by two independent healthcare professionals, a doctor and also a nurse, as required by law. (Notice then that the three cases here, Lancaster, Holland, and Dillon took place over years and not in the same few weeks they’re being, weirdly, reported in. And in those years there were tens of thousands of MAiD cases no one is complaining about and, without a doubt, countless hospital visits where MAiD did not come up in discussion or did not bother anyone...) The pair deemed Dillon eligible for MAiD under a recent provision established for those whose death is not immediately foreseeable but who are reasonably considered to be suffering intolerably from a grievous and irremediable condition. And, yes, he was driven to his final medical appointment by the physician. This was done because Dillon’s driver’s license was taken away due to his history of substance abuse, because he had no money, and because his family refused to take him as they didn’t support his decision — so, as far as I can ascertain, out of compassion and concern for this man’s basic human dignity.
In the aftermath, according to Ontario's coroner's death review committee and a subsequent College of Physicians investigation, the patient, Dillon, did indeed qualify for MAiD, was appropriately assessed, and was free to reassess and had plenty of time to do so. What the doctor was criticized for by his peers and overseers was what they said was too much communication with the patient (oh dear), his informal meeting with the man (seemingly at a time and place of the patient’s choosing, not a sterile office on the outskirts of town), and his driving the patient to his appointment (out of the aforementioned compassion) — so, for exactly the approach and standard of care we typically chastise medical professionals for failing to achieve. The physician was not charged with a crime, he did not have his license revoked, he was not found to have violated established MAiD protocols, nor was his work restricted in any way; instead, he was issued a caution and required to accept peer oversight for a period of six months as well as undertaking further education on informed consent and professional boundaries. All of that sounds pretty different from the grievous error or pure evil imagined in the reportage.
A TYPICAL MORAL PANIC
Why was all that readily available info left out of so much reporting and sharing? In all these articles, given people’s stated beliefs and their language and the abundant hyperbole, all paired with the fact that there are no formal complaints or even serious allegations in any of these cases, it seems to me like all these voices are radicals to some degree and attempting to arouse a moral panic (in someone's crusade to have everyone in society observe their particular moral framework and metaphysical worldview.) Seems pretty weird. Seems like an attempt toward a coercive and insensitive theocracy. Doesn’t it? I think so. How is it not? What else would you call this prescription for non-Catholics to abide by a whole spectrum of narrow beliefs around souls, the afterlife, and related theological tenets? And we might ask how these same voices would respond if these same assertions and wild accusations were coming from those of other faiths?
On that note, I think we’ve seen this many times before. Haven't we? Sadly, I see all of this rhetoric here as intended to foment the kind of rage that sends the committed and unhinged to kill abortion doctors and shoot up their clinics, for example, while preventing or making it increasingly difficult for people to get the help they need — paired with their failing to offer any realistic alternatives aside from ultraorthodox adherence. It’s disgusting.
So, you might wonder (or more likely you do not wonder at all) what happens when you point any of this out or note simply that the press and other serious voices are clearly misleading people by omitting details or getting some basic facts wrong? Me, I had thousands of people instantly telling me I am a “soulless communist piece of shit”, a “brainwashed sheep” and they hope I die and, my personal favourite, that their sincere wish is that “[MAiD] should take you too faggot.” These are our life-affirming moral superiors and spiritual guides.
CURIOUSER AND CURIOUSER
What’s strangest of all is that virtually none of these people, especially the fiercest opponents to MAiD, are actually against medically assisted death. Have you noticed this? They’re only opposed to you having any say in your life or your death. These folks know what happens to people in end-of-life care at Catholic- and other faith-run hospitals and hospices. They know the faithful are closely attended to and have their symptoms “managed.” That’s not a euphemism for “prayer” but the delivery of wanted and needed drugs. Out of pure compassion people are put on painkillers, anti-anxiety meds, and/or sleep aids. Those are intended to help patients comfortably endure the inevitable and excruciating critical organ failure that was diagnosed days, weeks, or months earlier. And if folks don’t hurry up and die those drug doses are increased (but always shy of actually relieving their pain or causing their organs to, indeed, fail.) Too often those drugs are still ineffective or deliberately restricted in this way so as not to kill and death happens very slowly, with one ceasing the ability to speak, gesture, or otherwise communicate far too long before one's final breath. But, of course, that’s just the experience on the side of the healthcare provider or the loved one. In this way they keep you alive and suffering, especially when they know you are suffering and have the tools to compassionately end your agony.
And what are the consequences of that? Anyone with any life experience — or anyone who has had sufficiently wild nightmare, scary trauma, or bad trip (or even anyone who has just read Einstein) — can tell you that time is, indeed, relative. What may look like moments on the outside or from afar may elapse over what feels like an eternity or just way too damn long for the person actually committed to the ride. Now, and this is what few seem to appreciate, what if you can no longer make the call and sign off on ending your own suffering (and cannot induce it by thoughts alone and no one you've mustered would do it for you) but are still very much alive and, even with all the meds in the world, the experience may be not merely torture but a profoundly uncomfortable and unremitting torture, where an afternoon experienced by those at your bedside is perceived to take weeks or lifetimes to elapse on your end? And what if, by the clock on the wall, the experience lasts another week (or 32 lifetimes)? If you’re ever engaged with someone having, or had yourself, a true emergency (a real existential crisis, serious night terror or sleep paralysis, a panic attack or psychotic break, or psychedelic-induced confrontation with the darkest side of the mind-and-multiverse) you may be able to appreciate the whole-of-Being urgency to remediate the situation — and know that there are places you can go where happy thoughts and well-wishes will not penetrate and cannot prevent your drowning (where it is just endless drowning and no conclusion comes.)
These opponents certainly won’t acknowledge that what they already offer is medically assisted dying — only with infinitely more needless suffering, less compassion, and less autonomy. I get no hint from those opposed to MAiD that they or anyone they’ve ever known has died a slow death or just looked into the abyss. And exactly none of them appear to acknowledge that, yes, faith and community and/or great healthcare and good meds can truly turn lives around but that they would deny people the greatest possible privilege: the ability to choose when and where, with whom, and why they die. And notice that no Catholic (or Muslim or Jew: those acquainted with scriptural sanction against suicide) would ever impose this torture on their pet fish or frog, cat or dog, but for grandma or their spouse it’s totally fine and makes perfect sense.
CHAPTER II - SEEKING, NOT SEEKING, AND THE CONSEQUENCES (REAL AND IMAGINED)
TRIGGERED
As if by Papal decree, all of this terrible reportage transpired alongside some of the biggest podcasts on the planet doing whole episodes — planned weeks or months in advance, doubtless — on Canada’s MAiD program. On May 23rd, for instance, the fellows at Triggerncometry did a show with guest Kelsi Sheren, who wrote a book on related themes.

Sheren is a self-styled “Somatic Breathwork Practitioner and Psychedelic Integration and Performance Coach” who, prior to her now-busy career as moral arbiter, deployed to Afghanistan as an artillery gunner with Canadian, American, and British forces and then did a stint as a jewelry designer, making fashion items from bullet casings… With this background, she informs us that Canada’s medical assistance in dying program is little more than Nazi-like eugenics operation with a cute euphemistic title and that, worse, doctors providing MAiD get paid exorbitant sums to incentivize their campaign of industrial-scale murder. Wow. And she goes on to explain that, now get this, the real motivation behind this program (in addition to the profit-making and delight at exterminating society’s physically, mentally, and morally unfit) is organ harvesting. I kid you not. She also tells us that things are so unhinged here in Canada that just anyone can order themselves MAiD in mere moments over the phone, as if ordering a pizza, and that she did this herself and shared the video evidence.
Sadly, much of what she says is pure nonsense (such as her friend who uses a wheelchair being “offered MAiD every day” or Canada seeking to kill off “difficult eaters”, “the vulnerable”, and “inconvenient.”) Alternatively, what she offers is on the order of anecdotal affirmations grounded in private personal conversations with her friends or otherwise the disgruntled tellings from the estranged or deranged family members of the deceased. So not the most reliable narrator or sources. However, the above are some of the few wild claims the guest makes that we can actually track down and interrogate. So, let’s do that.
ORDERING MAiD
Sheren tells her hosts the story of a young man, whose case she misrepresents, who got himself MAiD and had the final act performed at a funeral home. Sheren and others like to represent this case, of Kiano Vafaeian, as “a kid who had diabetes.” The reality is that the man was 26 and had been diabetic since age four. He had many complications as a result of his illness including blindness, serious eye pain, and significant nerve damage, with him describing numbness and severe pain in his arms and legs which seemed likely would leave him wheelchair-bound. He also suffered his whole life from notable emotional volatility, aggression, and depression. He had a very difficult time at school and was bullied. It is said that as a teen his behaviour became increasingly erratic. He attended and dropped out of multiple high schools before, at 17, he was involved in a significant car accident that left him with a concussion and serious chronic pain. His mother would not let him go on opioids but permitted a medicinal marijuana prescription (which, of course, is well-documented to pose a serious neurological and psychological threat to some males of this age.) We are told his mental and behavioural issues worsened further. His mother says he suffered “deep psychological distress,” that with all of his issues he was unable to hold down a job, and that he also became isolated. Kiano applied for MAiD in his home province of Ontario in 2022 and was accepted. His mother, now a friend of Sheren’s, discovered a confirmation email and launched a social media campaign to identify the doctors who made the approval and reverse the decision. That happened. In 2023, Kiano again applied for MAiD and was denied. In response, he and his family went to therapy together. Through that experience, his mother says that in September of 2025 she arranged housing, and a caregiver for him, encouraged him to join a gym, and told him “he could have all the organic food that he wanted, all the vitamins he wanted.” But at the same time he was applying for MAiD, one last time, this time in BC. In December of that year, while facing multiple criminal charges back in Ontario, including for drug-induced indecent exposure and also an altercation with his father, Kiano travelled to Mexico and then on to BC. His third MAiD application cited blindness, diabetes, and severe peripheral neuropathy as sufficient to meet the recently expanded eligibility criteria. He had his death carried out at a Vancouver funeral home.
Yes, Kiano’s case is truly tragic. And many people, on all sides, have very strong opinions about all of it. It does look like The System (his family, medical, psych, and education communities and on) failed him in all kinds of ways prior to 2022, and we can all see a hundred plausible interventions and preferable courses of action at every stage of his life. Fine. None of that should cause anyone to want to misrepresent the situation or pretend they know how the man felt, what he was thinking, or the outcome of their preferred course of action… Still, everyone seems to want to use Kiano as a political tool.
Horrified by this case, Sheren tells her hosts “I decided to call said funeral home and make a video about it. And I put it on Instagram.” In the podcast it sounds like she’s asserting that she ordered herself a medically assisted suicide and set a time and place for it, like Kiano, but right there over the phone. And it sounds like she and her hosts together wish to lead viewers and listeners to believe that, as a result, getting MAiD in Canada is no harder than ordering a pizza. She repeats the pizza line several times to drive the (false) message home and explains, “This just took a total of two minutes for me to organize a killing in a funeral home.” Except, if you watch her video, that’s not what happened at all.
Her social media post shows her call and enquire whether the funeral home provides a suitable space that may be used for someone seeking to receive MAiD. And the woman on the other end of the line, Rebecca, most certainly does not assume Sheren is seeking MAiD services, approval over the phone, nor that she is asking for herself. The staff member explains they can and do provide their “gathering room space for MAiD provisions” and are also able to offer related aftercare, regardless of whether that person wishes to use their cremation or funeral services or not. As Rebecca explains, given that not everyone wants to do this in their home or in a hospital. The video ends with Sheren’s call-long smirk transforming into glee as she hangs up the phone, turns to the camera, and says “You hear that? They’re killin’ people in funeral homes! Have a good day guys.” She really wants you to think, and repeat to others, that what we have here in Canada are tantamount to Nazi crematoria.

Clearly, if places of worship don’t wish to step-up, there are not a lot of other options; but a funeral home is an obvious fit and able and willing to contribute to filling that gap. I’d like to ask Sheren, “Where better?” and “Why are you so opposed to people having options?” The folks at funeral homes already deal with end-of-life stuff, have staff who are unhurried and sensitive to the sorts of expectations, decorum, and conversations that take place in such a setting, along with tending to have appropriate spaces that are quiet, private, and tasteful and can accommodate a dozen people.
Relatedly, in this podcast appearance Sheren also frames this service as part of a larger money-for-murder scheme. After hearing her misleading story, one of the hosts says to her “The more I hear about this, the more it seems to me that it's just about it's about money.” She replies, “A lot of it is.” In her call with Rebecca, she does ask if there’s a fee. Now she may find it inappropriate or downright appalling that a funeral home charge $300-$500 to accommodate someone, host their family and their friends for whatever time they need, and then hold, transfer, or deal with your body; but that seems, if only to me, perfectly within social and cultural norms and expectations and not a violation of all that is good. If I had been in the room, I would’ve asked “Do you also have a problem with a church or temple or funeral home charging $2,000 to host a funeral?” “What about this, exactly, sounds as demonic as you assert?” “You seem to want the room rental to be free but also, in the era of accessibility and accommodation, you want a very difficult or involve a lengthy process for someone (or their family or friends) just to rent a room? Should there be a multi-page paper form that needs to be filled out in person, taken and notarized, and then reviewed by a government agency, all with a requisite 90-day waiting period? Maybe a requisite IQ and sobriety test and credit rating evaluation? And all of that at no cost, too?” “What the actual fuck are you talking about?”
BUMPER CROP?
Another simple bit to verify and sort out is organ donation (aka “harvesting.”) We have good numbers on organ donation and info about how it works here in Canada and around the world. Canada, unlike much of the EU, has an opt-in organ donation system. While folks in France, Italy, Greece, Poland, Hungary, and across Scandinavia, for example, are donors by default under what is called a “presumed consent” regime, Canadians have to sign up to become a donor. I think that makes the whole argument that the government (or your GP or the town hospital or Big Murder inc, or whatever the argument is) is killing people off (only, almost exclusively the most elderly and unwell) for their body parts look like a pretty damned silly one. At least within an opt-out system, assisted deaths could conceivably yield transplantable organs that hospitals might not otherwise receive.
From there you might wonder where Canada sits among the nations of the world for organ donation. Surely if we’re culling the old and unwell at an industrial scale to harvest their livers and kidneys, as we’re told, you’d imagine we’d be near the top of the world’s donor list. But that is not so. Canada, it turns out, ranks right in the middle of the pack for deceased organ donation, with rates hovering around roughly 22 donors per million of population. This is less than half the rate of global leaders, places like Spain and the US, who are consistently between 40-50 per million people (and starkly ahead of everyone else, looking far more like organ harvesting operations are underway). And if you’re wondering, the US has an opt-in system like Canada while Spain considers every citizen an organ donor by default unless they formally registered their refusal prior to death.

It would be interesting to hear how Sheren or the Trigg' boys imagine the US or Spain achieve twice the organ “harvesting” rate of Canada — when she insists, and they nod in agreement, that Canadians are out here treating nursing homes and hospitals like factory farms. Do they think America’s hurricanes and school shootings are really just a front orchestrated by Spleen Harvest LLC or whatever? No doubt, all that was set up by Jeffery and the Israel Lobby, am I right?
If you want to go deeper into this, we actually have data on why people are applying for and getting Medical Assistance in Dying and those people’s contribution to our national organ donation system. The majority of folks (60-70%) who go through with MAiD have a terminal form of cancer and, due to both the risk of transmissibility and because of the drugs used to treat those folks, are ineligible to donate their hearts, livers, and kidneys — the very organs we tend to be most desperate for. Too, about 15-20% have chronic heart and/or respiratory failure. Those are not great organ donors, either. In all, recipients of MAiD account for only about 6% of Canada's deceased donor transplants; which means that without MAiD Canada’s organ donation system would be unchanged in world rankings.
Still, a recent study is said to have shown Canada was the nation with the highest level of organ donation among those providing medically assisted death. The press and others presented this, totally fraudulently just like Ms Sheren, with headlines and talking points such as “Canada Leads World in Organ Donations from Euthanasia.” And, as expected and intended, those unwilling (or unable) to read just started repeating this. In reality, the study included only four nations (Belgium, Canada, the Netherlands, and Spain) while omitting the bulk of those who’ve legalized MAiD (such as Australia, New Zealand, Luxembourg, Switzerland, Austria, Germany, Portugal, Italy, the UK, Colombia, Ecuador, and the United States.) From there, within their chosen quartet, researchers found a total of 286 people who sought euthanasia and also provided organs (to save the lives of another 837 other people). Almost half of those donors, 136 of them, came from Canada.
However, not only is this sample small, just a fraction of the global picture, but we might also notice that the nations examined are nothing alike, either, and Canada especially unlike the others in a whole bunch of important ways. The most obvious and least interesting fact is that Belgium, for example, is home to just 12 million people (four million fewer than are residents of the province of Ontario) and the Netherlands home to just 18 million. So it wouldn’t surprise anyone that there far were more MAiD recipients or organs donated in all of Canada, population 42 million, than in these two province-sized nations. And then to look at their MAiD-related organ output at a per capita rate (why would you be doing anything else?), both nations saw, relative to their populations, more donations than Canada. While Canada had 136 donations, at Belgium’s donation rate or that of the Netherlands we would expect to see a population of Canada’s size to be closer to 200 organ donors. That’s the exact opposite of how the data is presented. So why the all subtle misrepresentations and outright lies? Or, what am I missing and where can I find better data?
Just to be clear, ignoring organ donation, euthanasia has been legal in the Netherlands since 2002, more than a decade longer than Canada, and their rate of euthanasia deaths is around 54 per 100,000 people. In Canada the rate is about 41 per 100,000. And as far as organic, artisanal suicide goes, without the oversight or aid of medical professionals, places like the US consistently see far more, 20-40% more suicide, than Canada or the Netherlands. So what justifies this unique moral panic about Canada or assisted suicide?
LIKE THE NATIONAL SOCIALISTS OF GERMANY?
(I thought we agreed to not liken everything to Hitler or his most terrible works. What happened to that?)
So if the organ transplant rate in Canada is middling and the contribution of MAiD recipients to that number is happening at a rate significantly lower than some of our favourite countries, maybe the program at least resembles, in any way, the rapid eugenics-linked exterminations of mid-20th century Germany. After all, Sheren insists it does and gives us the numbers.
Talking about the scale of MAiD, Sheren says (in her overexcited, breathless manner):
Just to put it into perspective, when the Germans- not even the Holocaust, not even the Holocaust, not even the Holocaust, not even saying the word HOLOCAUST, here… -when the Germans went in and they euthanized mentally ill and disabled German population… All of World War II: 200,000 people! We're less than ten years [for 100,000 MAiD recipients in Canada].
Well, that has to be among the dumbest things I've heard on the internet. It's hard to even start with all the glaring problems of fact and comparison. For example, when I go to encyclopedia or museum sources to look up the timeline and impact of the German euthanasia program I find that it began in the Autumn of 1939. The operation systematically hunted down and, against their will, starved, drugged, and gassed people of all ages that the state deemed unfit. When the German public got wind of and balked at what was going on, in August of 1941 Hitler ordered a halt to the operation. At that time their own internal documents showed more than 70,000 had already been killed, just between January of 1940 and August of 1941, in six gassing facilities operating under the title “Aktion T4”. In reality a whole network of related operations carried on and accelerated. By August of 1942 German medical professionals and healthcare workers fully resumed the killings, only in a more clandestine manner and with broader scope to include bombing victims and folks in geriatric care. The program lasted right up until the end of the war, on May 7, 1945, when Germany surrendered unconditionally. Most historians agree this most gruesome Nazi side project took the lives of between 250,000 and 300,000 people, those the national leadership and medical community determined were unsuitable candidates for work or reproduction or simply too significant a burden on a society seeking purity and aiming toward utopia.

Sheren doesn’t just seem to think WWII and the Nazi clandestine murder program lasted generations, or something, and isn't just equating Canada's MAiD program (a transparent, voluntary, self-directed service for mentally fit, consenting adults who self-report interminable suffering) with a covert Nazi cleansing operation (that used misleading questionnaires to track down and pluck healthy babies and children from their families, recovering patients from hospitals and psych wards, and elderly folks and criminals alike; transporting them, entirely against their knowledge and will, to gas chambers or other facilities where they would be denied food or given lethal injections...) No. Not merely that. Of course, Sheren also misrepresents the number of people killed to attempt to make her ridiculous non-point.
It looks to me like all associated Nazi programs ran five-and-a-half years and killed roughly 275,000 almost certainly all unwitting or unwilling people of all ages and abilities. The MAiD situation in Canada is, very obvious, as close to the opposite of that as imaginable. Not only that but, out of 100,000 cases here in Canada (across a decade of legalized assisted death for willing adults seeking mercy), Sheren can't name a dozen instances where, knowing all the facts, she would do or even wish for anything different. Yes, there are a few individual cases where she personally, or the recipient’s mother or friend or some radical activists, didn’t like the scenario or feel there should have been other options. Okay. What none of those people do, as if they are all allergic, is: admit they don’t have all the information; concede that they don’t know the minds or experience of those who self-reported interminable suffering, or; fairly represent those tiny minority of cases.
FOR-PROFIT?
(Now, we won’t get into how this artillery gunner had no problem, herself, killing people for money and career advancement… And we won’t get into how it appears she doesn’t want doctors to get paid to do their jobs…) As you probably know, medical assistance in dying didn’t start in Canada or in the 21st century but in Switzerland back in 1942. In Canada, the program is a legal medical service and all doctors in Canada are paid, like any other, for providing their services. With MAiD patients, as with all others, doctors are paid for the complexity of the issue and time spent reviewing medical records, for interviewing their patients, and for ensuring medical safeguards are met. None of that seems crazy to me. How would you rather things were run?
The first thing to point out here is that when MAiD first came in, doctors complained they were discouraged from helping people because they were so underpaid for the service, some claimed they were getting closer to minimum wage, as low as half the rate of standard operations, for hours of labour.
From what I can tell, today in British Columbia a doctor can bill the healthcare system an assessment fee of $350-$900, depending on the complexity of the patient's condition and how much work goes into that assessment. As with any other situation, a doctor may also bill for prescribing medication, taking time to explain legal waivers to their patient, or for travel time for in-person home visits. Then the administration of the lethal medication is billed as any clinical procedure, at about $200-$455. So the total fee could come out somewhere between $800 and $3,000 per MAiD patient. No part of that seems like an obvious crime or something sneaky going on. And, obviously, all doctors have a right-of-refusal if they have a moral objection to providing these services and see themselves as a conscientious objector.
By the podcast guest’s evaluation and arithmetic, there are Canadian doctors earning themselves on the order of $860,000 for “killing over a thousand people.” She doesn’t explain her math, tell us where her numbers come from, offer how many physicians are at that level, over what timespan they accrued that sum, where they are, or who they are. Naturally. Given that, it also shouldn’t surprise you that neither she nor her hosts notice or spell out for listeners a totally plausible scenario that works with her numbers, such as: seeing two patients per week for ten years and earning what a mid-career teacher makes for that. Are we talking about the same thing? I don’t know. If we are, that doesn’t seem like the unimaginable windfall she’s making it out to be. And, of course, regardless, we know OnlyFans models and basketball players who make $800k on a weekly basis, so Sheren’s MAiD doctor scenario doesn’t seem quite like the extreme figure or incentive to murder she claims it is.
Related to this, we might ask why some people may be earning “a lot” of money performing MAiD-related services. Well, how about the obvious fact that many physicians use their right-of-refusal to opt-out of providing this long-standing and fully legal service on religious or personal ethical grounds. Why not notice, then, that it is precisely those doctors who don’t wish to help people who are suffering who push more work to those willing to do so? And why not notice that in the absence of MAiD, Canada’s wealthy and globe trotting elite were, for 80 years, making use of the service overseas and would do so again if MAiD was, itself, killed — that the whole system is just here to provide Canada’s poor and middle class with the same end-of-life autonomy and care as those able to buy a pair of first-class plane tickets to Zürich and a week in a suite at the Baur au Lac? Why ignore everything while pretending to deliver a comprehensive overview and critique?
I mean, look, if Sheren cared about for-profit medical exploitation she might contrast the fees collected by hospitals and practitioners for a MAiD death in Canada with far more ubiquitous and uncontroversial services like baby deliveries in the US. While effectively free in Canada (and throughout the developed world), an unproblematic vaginal birth in America (of which there are around 2.4 million per year) can average between $6,000 and $16,000 ($22,000 Canadian). A caesarean section or any kind of complication requiring the services of a neonatal intensive care unit (1.1 million annually) can start at $15,000; but, of course, there’s no upper limit and just the average tends to be on the order of something like $225,000 USD (or $308,000 CAD). As we all know, many Americans are without health insurance and those on plans offer wildly different coverage, meaning the out-of-pocket cost can vary as wide as possible. There's a famous case of a couple from Saskatchewan going on a trip to Hawaii and giving birth prematurely, and then finding themselves on the receiving end of a bill for $950,000 (and, as you'd expect, their travel medical insurance gladly opting out of paying anything.) Just getting a few stitches in the US, as my wife can tell you, can cost $1,500 with insurance or $5,000 ($6,900 CAD) without, so I don’t know how anyone could frame MAiD in Canada as an egregious profit-seeking endeavour and global disgrace — when it happens to so few and at practically no cost and with so little paperwork and, thus, so few billable hours.
If you don’t like that, consider the fact that the above fees for service can only be charged one time. As such, this conspiracy hypothesis, at least as stated, makes no sense. As far as I can tell, MAiD fees here in Canada would be comparable to cataract consultation, surgery, and follow-up (on just one eye, not two). And maybe you’ve noticed there’s no aftercare or follow-up with MAiD. Obviously that seriously cuts down on a doctor’s fees for service. So almost anything would be better than MAiD if a doctor was solely motivated by money, as the argument goes. Why not at least get a patient on some long-term experimental drugs and into multiple therapy or counselling programs or into some kind of long-term care or housing program (maybe that you own and lobby government to endorse and fund with tax dollars)? That be, what, $10,000-$20,000 per person, per a month?! I can think of all kinds of business and get-rich schemes of this sort all day long. And I don’t see why anyone with a profit motive would cut all that out, at least twice the money, prematurely. So, as you can see, MAiD is probably the worst way for a doctor to “make money” and must be the least considered argument. That's especially true when any Canadian physician could effortlessly migrate a few kilometres south to the US and they can easily make twice (or 50X) the money just prescribing pills (especially monoclonal antibodies) to Americans, where some doctors earn millions, and even tens of millions, doing so. Make any of this narrative make sense. I dare you!
CONFLICTING CLAIMS
From there we can point out some missing links or contradictory arguments. We’re told the evil non-Conservatives are trying to purge society of the weak and unwell in typical eugenics style, for instance. They say the medical system is trying to off difficult or chronically ill patients who are said to be a costly burden on the system. Does that jive with anyone’s experience or any story we normally tell about these systems or the people who run or are served by them? Not as far as I can tell.
Isn’t the typical story that Big Pharma (in cahoots with the WHO, public health, hospital administrators, doctors, and, of course, Bill Gates and maybe the telephone companies and the interdimensional aliens who live at the bottom of the sea) wants to cure nothing and instead keep everyone on drugs and relying on evermore elaborate medical services to wring every last nickel out of struggling taxpayers? How does swiftly rounding up and bumping off all the ill, infirm, and elderly (none of which is happening) achieve that end? I don’t think it does.
And then you have the fact that Canada and countless institutions herein are renowned for pouring endless sums of money and resources into “supporting” people with addiction. Our “harm reduction” programs (which I only really have problems with) are more numerous and well-funded and have been running longer than almost anywhere else. So, for example, the street value just for drugs alone (not the tools to test them or use them or for overdose prevention or anything else) can be to the tune of hundreds of thousands of dollars per person per year. Those prescribed pharmaceutical-grade hydromorphone, for instance, can collect 28 pills a day, every day, worth between $2 and $30 per pill depending on where, by, and to whom they are sold. This is precisely why organized crime inserted themselves into the scheme. No part of that suggests an institutionalized attempt to purge the unwell or any effort even to reduce spending or to coerce or merely adjust the behaviour of those among us who are not someone’s version of ideally well-rounded and well-adjusted. The opposite really. Seems we, almost unique in the world, will go to nearly any length to avoid anything approximating coercion.
So eager to protect these best friends of the meth and fentanyl producers and keep them on their product forevermore, right at the start of the pandemic provinces and municipalities in Canada dropped hundreds of millions of taxpayer dollars buying up Howard Johnsons, Comfort Inns, and local motels as emergency housing for the “unsheltered.” (“Are you really ‘unsheltered’ if you curl up every night in the stoop of a shuttered cannabis dispensary in a wet sleeping bag with your head covered by half a waxed lettuce box you got for free from the Vietnamese restaurant across the street?”) In BC we spent more than $220 million to “shelter” 810 people (or $272,000 per person) in the first year of COVID and then dropped another $200 million the following year. (And none of that was the cost of assisted living or any kind of care, just real estate, and typically nothing more than a tiny, shitty motel room…) The feds also launched a billion dollar program to do the same or to lease properties to the same effect across the country. Someone should ask Sheren why we didn’t do nothing, instead? Or why everyone didn’t make piles of money by bumping these people off, these most burdensome among us, and then harvesting their organs in our national for-profit, Hitlerian eugenics and pancreas-laundering scheme? Beats me.
It’s also worth noting that none of these expenditures are really a financial burden on society as even the billions spent annually just here in BC interrupting or addressing “mental health and substance use” is only a fraction of what is otherwise lost in terms of productivity, health care costs, criminal justice, and more. Spending a billion to save two or three doesn’t seem like a terrible investment. And alcohol and tobacco are far more burdensome on society than all other substances combined…
I hope you can see that anyone spreading the kind of messaging you hear from Kelsi Sheren is a true radical and someone unconcerned with reality.
ANOTHER ANGLE
On May 26th, 2026, the day after the Triggernometry podcast landed, The Free Press published Coleman Hughes’ podcast interview with Rupa Subramanya, also a contributor to The Free Press, on the same theme of MAiD in Canada. On his podcast, Conversations with Coleman, Hughes reports being sensitive to the issue and supportive of the right to die for terminal cases — and shares that he lost his mother to cancer and gained an appreciation for the mercy of assisted dying due to the fact that her pain from metastatic bone cancer was both brutal and resistant even to the most potent opioids. Hughes tells us, however, he is nonetheless troubled by the path he feels Canada has taken with assisted dying. Subramanya shares this concern. She explains how “Canada’s medical assistance in dying program should alarm even right-to-die supporters.”
I like both these folks and follow their reporting and feel this particular conversation benefits from not being full of BS; still, I disagree with much of what’s offered and have questions about most of their key points, arguments, and explanations.

First off they tell us that we’ve seen the policy of legalized self-euthanasia “explode” in Canada and expand far beyond its starting place and the selling points of a narrow and cautious framework aimed at unambiguous compassion for a select portion of those in the final moments of terminal illness. Subramanya explains how the original and much more limited program, established in 2016 and directed at those whose death is “reasonably foreseeable,” was broadened, as she says “dramatically,” during the pandemic to include cases where an individual is not terminally ill and with an imminent death but to include those with severe physical illness or disability whose “suffering is considered intolerable.”
I still don’t really understand what the argument is. Obviously restrictions and layers of oversight are essential to this program, but we are all going to die. And, as I argued earlier, by my estimation and that of many others, there are worse things than dying and sometimes far worse things than dying soon. One of those things can be not dying. Another could be not dying soon enough. And I’ve never heard a serious argument to the contrary. It continues to sound to me like folks hold some weird kind of naturalistic fallacy around death that says if human agency is involved it must be inherently bad… or something. And while they aren’t opposed to MAiD, nor are they raising awareness about or seeking to reduce traditional, unassisted suicides, folks are (more of less) opposed to assisted death for coherent consenting adults going through what I assess to be the worst cases of human suffering that can be named.
THEORETICAL CASES
Subramanya then explains that there is a further expansion of MAiD pending, one that promises to take what we are assured is already far too broad and permissible a schedule and allow for assisted death for those whose “sole underlying condition is mental illness or psychological suffering.” Well, okay, hold the phone. She offers an example for someone who, she says, might meet this new threshold for MAiD: “you could be in a wheelchair for the rest of your life and if you find that suffering ‘intolerable’ you could be a candidate for MAiD...” Now, she doesn’t provide a single example of this within the existing cohort of what we are told by others is “nearly 100,000” cases. (Though she does later bring up the example of Kiano, which does seem like our worst case mostly for his youth. But, like everyone else seemingly, she tells us he was someone “with diabetes who was blind”, which excludes much and I find seriously misleading.) So is that actually a concern? Are Canadians even applying (and being rejected) for assisted dying after having read the new rules and figured that they fit the bill because they consider their height or eye colour or a lost limb or what they see as an insufficient number of Tinder dates to be ‘intolerable’? Why bring it up unless there’s a single incident of this or you can share doctors, those you are happy to name and who are happy to be identified, who report real concerns that Canadians feel this way and are trying to apply to be killed with the help of a pair of doctors for normal, everyday life stuff or moderate and momentary annoyances?
Also, you know that folks can just walk out into traffic or off the viewing platform of a skyscraper, right? And every bed-stricken hospital patient can choose to stop accepting food and drink, right? And there are on the order of 4,000-5,000 of those annually, right? And that the rate of suicide significantly declined from peaks in the 1970s and ‘80s, right? If anything, it seems to me MAiD is less than a slippery slope to mass suicide and more like it is or could be a slippery slope to vulnerable people having a serious conversation with a trained medical professional. After all, unlike government issued prescription-grade opioids, meth, or cocaine, you still can’t get free MAiD drugs from a vending machine or street activists. And, to me, the key to avoiding problems in this domain would be relieving any doctors of their duties if they’re found to be doing something other than promoting life and wellness… (I guess I have to keep repeating that.)
BETWEEN LUCID AND GONE
I guess I just don’t know what planet people are living on. As far as I’m concerned, mental illness or psychological suffering is all there is to be worried about and the real domain that needs addressing. The other stuff is the easy stuff.
It is true that pain is not concrete or well-defined and is something far more complex and persistent than anyone would wish it to be; but pain, I think we all agree, is very real. Something like 20% of adults are inflicted with chronic pain. Chances are that if you don’t have chronic pain yourself you know someone who does. It is also true that pain is the thing many nearing death or applying for MAiD report being worried about and are seeking to avoid. However, I’m convinced that is misguided. Seriously misguided.
For most people in most situations, physical pain has not been an unaddressable problem since the discovery and distribution of any number of substances and concoctions, particularly those potent alkaloids such as opium (enthusiastically cultivated since the dawn of civilization, around 3500 BCE) and its more recent derivatives, of which there are many, such as: morphine, codeine, heroin, oxycontin, hydrocodone, fentanyl, methadone, and the like… And pain is far less of a problem in the 21st century, and even less so in a clinical setting, than at any other time. That is to say, even looking at terminal cancer patients, the vast majority (70-90%) are not like Hughes’ mother (peace be with her) and in that category of those with severe “refractory” pain unmitigated by standard analgesic medication. (But even for the minority with pain that refuses to be dampened by opioids, palliative care teams today can figure out work-arounds that make use of procedures to target nerves directly…) My father, for example, had terminal cancer, was seriously worried about pain all along, and was someone for whom well-administered pain meds did appear to work. Still, my own life experience and time with my dying father convinced me that the perfectly logical and understandable focus on pain, and also with the natural self-preservation that is a concern for ending one's life “too soon”, is, however reasonable it seems, deeply confused.
The truly scary place, as mentioned before, is where my father allowed himself to go despite a terminal diagnosis and all the concern in the world for his own potential suffering. Even with the end in sight, one simply cannot know when or how they will transition across that point-of-no-return from lucidity and volition to something other. And there is no clear line or any view of such a line at any point, only the stark realization that a transition has been made and there is no going back. So — even if you have a do-not-resuscitate order, and get yourself approved for MAiD, and everyone knows your intentions are clear, and you have the meds sitting next to you — it may just be that if you don’t pull that trigger “too soon” it’s probably already “too late.” But, actually, it’s worse than that.
No one can know the time or distance (real or imagined, neither from the experience of your own subjective self nor that of your loved ones or healthcare providers) between that loss of outward autonomy and ability to communicate (which can just… happen) and what those of us who’ve never taken that ride perceive as the “end of this life.” As noted earlier, though no one else seems interested or concerned about it, I don’t think you could convince me that:
A) The the journey from lucid to gone must be brief (or that it could not last a subjective eternity), and
B) It must be pleasant (or could not involve a level of suffering orders of magnitude beyond what anyone would ever wish to endure)
I mean, I get how if you believe in an afterlife you may have faith that, as you have lived well in this life, the life-after will indeed arrive. But even with that expectation, I’m not sure how you convince yourself that there are not whole eternities, and at multiple stages, between here and there. I see that voyage looking something like this: Normal life -> being alive but losing the ability to communicate [potential black hole] -> loss of perception [potential black hole] -> loss of consciousness [potential black hole] -> death [potential black hole] -> your heaven.
I don’t happen to believe that’s the universe we live in; but, still I would love to know where this is covered in the Enūma Eliš or the Upanishads or Old Testament? Does Rumi or Guru Rinpoche, William of Ockham or Laozi get into this? Where do they convincingly cover this most elementary set of concerns that, by my evaluation, surely anyone with a nervous system has been forced to ponder? You’ve never had a spooky dream or nightmare, sleep terror or sleep paralysis? Kittens and chickens do… And where are the pharmacologists (no doubt conspiring with some college-aged reincarnation of Terence McKenna and a 200-year-old woman they found on the muddy banks of the snakiest bend of the Juruá River) who’ve concocted the potions to address this, or merely look it in the face and report back?
No. If you think your ketamine or N,N-Dimethyltryptamine touch this I can assure you we’re talking about different things. I’m not talking about you setting the stage, being appropriately hydrated, wearing your favourite comfy-pants, finding a relaxing position, being amongst your friends or trusted psychonaughts, and then transcending your body and perhaps Space-Time for what feels to you like hours or months or three lifetimes but, to everyone else in the room, elapsed over 26 minutes. I’m talking about what is effectively the opposite of that.
Imagine being in a terrible setting, far from comfort and perfectly disturbed, thirsty and hungry, too. And now imagine we strap you down and pump DMT into you, every minute of every day for a week or more (by the clock) or until you die. If that’s inconceivable, I strongly encourage you to try and conceive of it or let me help you do so.
Objectively so, many people wind up in hospital or hospice entirely before they would ever wish to be there. And often suddenly, by surprise. And, just as often, there is nothing pleasant about what is going on or the experience of that. And in such environments, as you know, problem-solving (and just doing stuff) is the name of the game. Typically, if a patient has any information to offer or anything to complain about (both of which are pried out of them by man and machine alike who are often there for this sole purpose), all that doing potential energy has somewhere to focus and go. And, let me assure you, if there isn’t a reason to x-ray or scan or put you in a machine or on a pill or a drip or to intubate you or shock you back to life (or to kill you and shock you back to life again) someone will almost certainly find a reason.
DAVE
My father, for example. I’d just spent a week with him. He was up and about as usual, driving around, going out for dinner… If you’d asked I would have assumed he had another decade or two in him. But shortly after I left he went to the hospital after having a fall. (Or, this is how it was relayed to me.) Then someone decided they were keeping him there for a little bit. He had some bleeding and bruising that was not an emergency exactly but, because he had cancer and been on blood thinners for years, they needed to monitor for a bit and sort things out. Then, out of nowhere (being in a hospital), he was gifted with pneumonia. After a couple of days, suddenly, one of his lungs collapsed. (And then I’m getting a phone call that I should probably get to town, real quick.) And then things went sideways and he was having heart and lung issues and, oh, he died but they’d shocked him back to life; however, though his lungs were sorted out, he came back with an unsustainable and erratic arrhythmia. And then they wanted to put him out again and try shocking him back to life to try and reboot his heart. (Or, this is how it was relayed to me.) I don’t know if they did that. What I do know is that in no time he’d signed a DNR and a few days later he and I were riding in the back of an ambulance, off to a hospice, the one some of my other family had ended up at previously.
There, over days (I actually don’t recall how many but way too many), he received every kind of drug to ease and hasten his end (but not too much, because that would be “murder.”) As I said before, I think the pain meds worked pretty well. For the first day or two he was chatty and wanting to see people and was as fine as could be expected. (Though he said some crazy shit that will have to wait for another essay…) But was he sleeping? Not really. Yes, despite the sleep aids. Did he report or seem comfortable at any point? Also no. Why would he be? But he wasn’t in “pain.” He wasn’t blissed out, either. You can, quite clearly, be in a place opioids and anxiolytics cannot reach. As time went on, between bouts of being drone-like or half-sleeping, he was extremely frustrated, anxious, occasionally mad and afraid and sad. At least that was the case when I was in the room. He was also clearly, at minimum, really dehydrated. And that went on for days. That was his baseline. Eventually he stopped talking and opening his eyes but was still responsive. And he was in that state for days and what my whole being told me was way, way too long (even just on my end).
The whole time, as his discomfort increased I was pleading with the staff to up his meds or see what they could do for him. I believe they did everything they legally could, and they told me as much, but never to any obvious positive result on his end. And I most certainly didn’t feel like he was in a good place physically or psychologically. I didn’t feel like there were any positives that came after leaving the hospital (or at the hospital, for that matter). It seemed to me that no soul would want this for themself nor would anyone ever put their dog through any of it. But, of course, there was no obvious point to interject or, short of murder, no action for anyone to take. If anyone was going to do that he needed to do it for himself. (And that’s what MAiD is.)
Again, if with the slightest deviation from normal experience can make half an hour feel like way-too-damn-long or a literal eternity, then how long does five or 12 days last? Just 300 eternities? Plus or minus the elapsed lifetimes of a hundred universes? Can you at least see what I’m getting at?
At some point I was no longer able to take it. Psychologically, I just couldn’t tolerate the situation and I actually left and went to a friend’s house for a day. I had to get out of there because it felt like we all were torturing him for no reason, neither keeping him alive nor ending it. (And he had kind of done that to himself, too. By seeking to avoid ending it “too early.”) To me, what was happening seemed pretty far from what he would want or what anyone else could rationally call compassion or even anything anyone should consider normal, never mind feel good about.
But one morning before dawn, while my brother and I were spending the night with him, he finally took his last breath. At that point I wasn’t sad. I was overcome with the feeling of relief. I was glad. Though I could make sense of it, it was a very disorienting feeling for a non-psychopath. And I really hated that. Even if I’d hated the guy every day of my life, I don’t think I ever could have mustered that feeling. I felt like, for our collective lack of consideration, he, and the medical system, and I suppose our whole culture, made me feel overwhelmingly relieved that my father was dead. And the whole experience left me with the sense that this is the kind of collective psychosis we demand and import into the world, and inadvertently gift others, by not considering what we know to be true while also preventing or overly restricting MAiD.

That is to say I think there are all kinds of reasons to suspect at least one unarticulated black hole may await under some circumstance and likely experienced by many. And, to the point, I also think that provides a pretty robust reason to believe MAiD (or any number of alternatives) can take you beyond the pull of that event horizon to where you wish to be (whether that’s just lights out; basking in the Beatific Vision; residing as a gidim with Ereshkigal in Kur; in the highest of the 13 heavens, Omeyocan, with Ometeotl and his warriors, or whatever it is...) And I think there’s an argument that that is what you want. So, as you can see, I think it’s ludicrous to emphasize “pain” or to reject the primacy of the psychological (which was obvious long before Descartes, but at least by his time). And, as such, I also think it is senseless to allow MAiD only for those with certain species of terminal illness or who are at a certain stage toward death. To me that’s bonkers.
A PROBLEM OF INDIVIDUALISM?
After sharing their concerns about expansion of MAiD accessibility, Hughes asks, “I'm curious, what is it about Canada's political culture, what beliefs and values are in the air, such that so many people seem okay with the expanded policy — which most places on Earth, I think, would be a non-starter?” Subramanya replies by sharing her evaluation that, as someone from India, she views Canada, like many Western countries, as an “intensely individualistic society that places autonomy at the center of life” where suffering is “no longer seen as something you endure collectively or spiritually” but alone or maybe with the help of the state.
Though this is a popular stereotype, I’m not sure that the data on suicide supports the claim. To begin with, surely medically assisted suicide is less solo and individualist than conventional forms. And many places that are the most collectivist and/or where the state religion forbids or at least strongly frowns upon self-directed death of any brand or flavour — which is much of the world — we just don’t have a good sense for what’s actually happening. But where we do have numbers, what is revealed is that it is often those most interconnected or communal and most religious or spiritual places that have the worst suicide rates.
So, for example, the per capita (per 100,000 population) suicide rate is the worst in Africa. It’s particularly bad in those places with a tradition and language around the concept of ubuntu (or interconnectedness, often translated as “I am because we are”) such as in Lesotho and Eswatini (with ~28 per 100k) as well as Suriname and South Africa (at around ~22 per 100k). Over in Asia, places such as South Korea (guided by jeong), Japan (infused with wa, giri, kizuna, nakama, omoiyari, and seken) and Thailand (grounded in samānatatā, paticcasamuppāda, and nam jai) have suicide rates between 15 and 21. And in the West, the US, France, and Belgium are in that same range as across Asia, while Canada, like the UK, sits at closer to half that rate, bouncing between 9 and 11 per 100,000. And, in case you’re curious, the lowest reported suicide rates, which seem fictional by my reading, are mostly in places where stigma is highest and taking one’s own life for any reason or by any means is deemed a cardinal sin, like in Indonesia, Pakistan, Jordan, and Saudi Arabia. I just don’t know anyone who would claim that the Indian sati, the practice of Hindu widows self-immolating on their deceased husband's funeral pyre (or being set on fire by others), or the Japanese kamikaze pilots or jihadist suicide bombers all suffered from too much self-concern and/or too little spiritual conviction. That is kinda the argument coming through in this podcast, however. Something like that.
A PROBLEM OF HEALTHCARE PROVISION?
The other assessment on offer for why Canada is so crazy and Canadians so eager to kill themselves and one another — none of which is borne out in any data I’m looking at — is that timely and/or quality healthcare are not to be found here, or at least are consistent problems pushing people into MAiD when they might live a little longer.
There are criticisms to be made of Canada’s wait times or barriers to access or any number of things, but compared to who? If, for instance, you go read the Commonwealth Fund’s 2024 independent evaluation of health care system performance, America lands dead last among 10 peer nations. In the broad categories of access and outcomes, the US is the worst and they only climb up to second worst for administrative efficiency and equity. But even that obscures the facts. What’s really stark in their assessment is how every other nation is roughly on par in many areas while the US is practically off the charts for how poorly it performs, especially on people being left out of the system and what folks spend relative to what they get. So, if poor outcomes, difficulty navigating the system, or lack of access causes people to lose hope and opt into MAiD, why aren't America's state-level assisted dying programs overflowing or its suicide rates double what they are?

It's true, Canada isn’t leading the world or anything, it ranks 7th overall among this group, but places 4th for outcomes and care process and 5th for administrative efficiency. That said, unlike America, even where Canada lags behind in areas it mostly remains close behind or alongside peer nations like Sweden, the Netherlands, France, Germany, New Zealand, and Australia.
And, again, effectively everyone who has received MAiD in Canada has been in a bad way at the end of their days or with profound problems that community, faith, and medicine have no way of alleviating or reversing — and not awaiting a liver or fMRI scan they just couldn’t afford or get. I would also be willing to bet that will continue to be the case.
CONCLUSION
It’s highly curious to me how these stories and conversations all came out so close together. And I don’t understand why the reporting is so poor or the push-back so weak or absent. All in all, my only hope in pointing some of this stuff out is that maybe we can upgrade our discussion of these themes, themes I think are hugely important.






























































































